This is a ‘bleeding obvious’ statement. It is well acknowledged that malaria is a disease of poverty addressed in this column on June 13, May 9, April 18, February 1, October 6 2024 and June 29 2024. Malaria disappeared from Europe, North America and much of Asia as living standards improved.
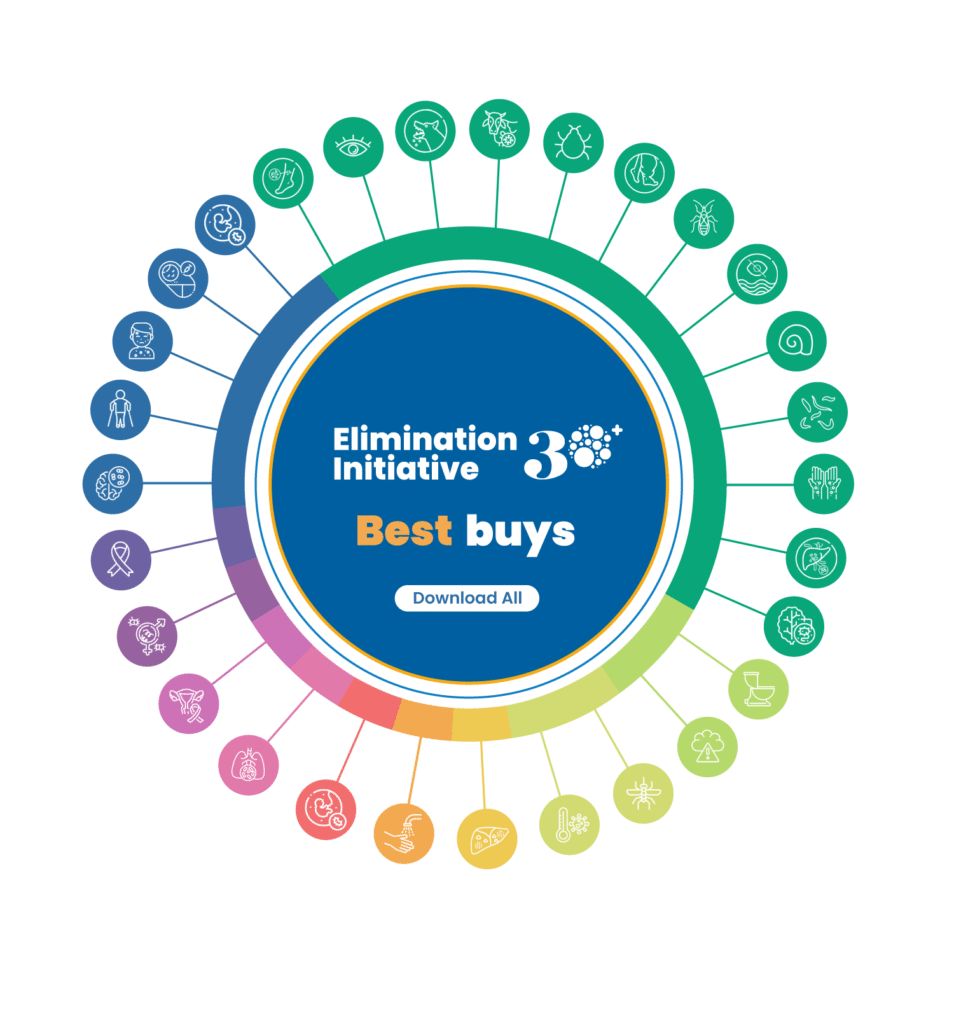
And, of course, money is the fuel that keeps the malaria research and treatment business going, which is probably the motivation behind some articles in MalariaWorld this week. One article from PAHO, Pan American Health Organization, which is WHO in Americas region is ‘Best Buys to accelerate disease elimination in the Americas’.
PAHO has developed Best Buys, evidence-based technical briefs that summarize, in a single page, the most cost-effective and high-impact interventions recommended for each disease or condition. The attractive website has a wheel and you can click for any individual disease or all.
What does it say about malaria? The ‘Best Buys’ just seem to be business as usual. Is this approach solving malaria?
- Expand access to early diagnosis and treatment:
- Ensure universal access to diagnosis for suspected cases using rapid diagnostic tests (RDTs) or microscopy
- Provide timely, barrier-free diagnosis and treatment in all endemic-area health services
- Engage communities in testing with RDTs for early diagnosis and treatment
- Adopt strategies to improve radical cure efficacy or effectiveness for Plasmodium vivax uncomplicated cases
- Prevent transmission:
- Distribute long-lasting insecticidal nets free of charge in endemic areas
- Consolidate malaria-free micro-territories:
- Use microplanning to expand access to services and consolidate malaria-free areas
- Innovate in supervision and logistics using information and communication technologies
- Accelerate elimination at the subnational level and pursue subnational verification of elimination
- Strengthen surveillance to eliminate and prevent re-establishment:
- Maintain strong surveillance systems to detect and treat imported cases in all malaria-free countries
- Use data and information to guide local-level decision making and action
The second MalariaWorld article is a blog post by Duma Gideon Boko, President of Botswana and Chair of the African Leaders Malaria Alliance (ALMA), titled ‘Why ending malaria depends on bold financing and global leadership’ in Health Policy Watch. The core principle of the article is that more international funding is needed to pay for mosquito nets, treatments and diagnostic tests. Somehow economists calculate that each dollar ‘invested’ in malaria yields four in economic activity.
Africa will solve malaria the same way the rest of the world did, by lifting everyone out of poverty. Malaria disappears when nutrition, water and sanitation improve. However, this is unlikely to happen as long as African leaders such as Boko continue to emphasise appeals for money from the former colonial powers to pay for nets, drugs and tests. As for African leaders, for every Traore there are at least 10 Bokos.